Addressing Discrimination Supports Youth Suicide Prevention Efforts




Suicide is the third leading cause of death among youth ages 15 to 19 and the second leading cause among youth ages 10 to 14.[1] As state health and education leaders work to address the health effects of the COVID-19 pandemic—including those related to mental health—they should examine patterns of suicide risk across different groups of youth. For example, the percentage of Black, Indigenous, and other People of Color (BIPOC)[2]; lesbian, gay, bisexual, transgender, and queer/questioning youth (LGBTQ)[2],[3]; and youth with disabilities[4] who report suicide attempts is higher than that of their peers. Experiences of identity-based discrimination are associated with increased risk of suicide, especially among youth with multiple marginalized identities.[5] To effectively reduce suicide among youth with the highest risk, state leaders must understand the relationship between discrimination and suicide risk. State leaders must also support efforts to reduce exposure to discrimination among youth.
This brief summarizes youth suicide risk patterns from recent nationwide surveys, highlights variation in suicide attempts across states, and reports findings from a review of state suicide prevention plans to determine whether they address discrimination as a risk factor for youth suicides. Tables at the end of the brief include 2019 Youth Risk Behavior Survey (YRBS) data on suicide attempts by race/ethnicity and sexual orientation to enable comparisons across different groups within and across states.
Download
Much of this brief’s data on youth suicide risk come from nationwide surveys on adolescent health conducted by the CDC in 2019 and 2021.
The Youth Risk Behavior Survey (YRBS) is conducted by the CDC every two years. The most recent data are from 2019. The YRBS provides estimates at the national, state and local levels that allow participating states and districts to demonstrate how the behaviors of their youths compare with those at the national level.
The Adolescent Behaviors and Experiences Survey (ABES) was conducted by the CDC from January–June 2021 to assess student behaviors and experiences during the COVID-19 pandemic. ABES was a one- time, probability-based online survey of U.S. high school students. Estimates are available at the national level, but not the state level.
Suicide attempts among youth vary across states.
Nationwide, nearly 1 in 10 high schoolers report a suicide attempt in the past 12 months, according to the 2019 YRBS. However, that number varies by state. In 2019, the percentage of high schoolers reporting a suicide attempt in Alaska—the state with the highest percentage nationwide—was more than three times the corresponding figure in New Jersey, the state with the lowest percentage. Examining state-specific data, as opposed to relying on national averages, allows state and local health and education leaders to better tailor their suicide prevention efforts to the needs of youth in their states.
Percentage of youth reporting a suicide attempt in the past 12 months, national average and states with the lowest and highest percentages.
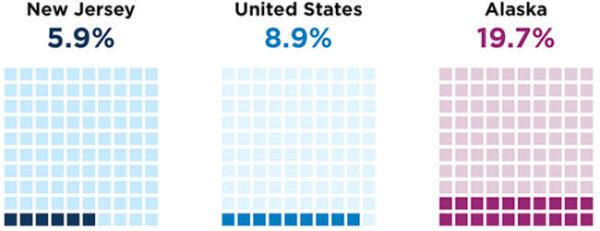
Source: CDC YRBSS, 2019
Suicide Attempts Among LGBTQ Youth
Suicide risk is higher among LGBTQ youth than among their heterosexual and cisgender peers.
The percentage of youth who identify as lesbian, gay, or bisexual (LGB) and who report a suicide attempt in the past 12 months was more than 3.5 times higher than their heterosexual peers prior to the pandemic, according to 2019 CDC YRBS data (in dark blue below). During the pandemic, the percentage of LGB youth reporting a suicide attempt in the past 12 months was five times greater than their heterosexual peers, according to 2021 data from the CDC ABES (light blue).
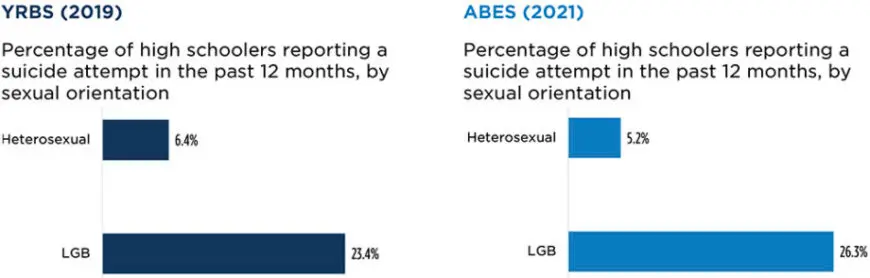
Source: CDC YRBSS (2019); CDC ABES (2021)
Both surveys include a nationally representative sample of youth. However, the ABES was a one-time, online survey while the YRBS is an ongoing paper-and-pencil survey completed in school.
Few sources of nationwide data examine the risk of suicide among transgender youth. For example, there are no nationwide data on the rate of suicide deaths among transgender youth. However, in 2017, 10 states and nine urban school districts piloted a gender identity question in their YRBS administration and found that the percentage of transgender youth reporting a suicide attempt (35%) was 4-7 times higher than among their cisgender peers.[6]
Percentage of high schoolers reporting a suicide attempt in the past 12 months, by gender identity
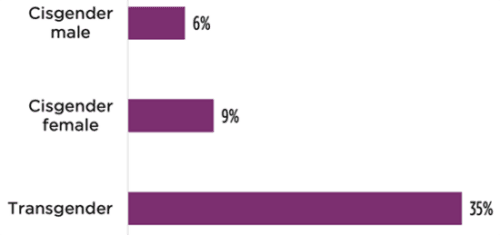
Source: Johns et al., 2019
Among LGB youth, the percentage reporting a suicide attempt is highest among youth who identify as more than one race.
Similar to the pattern observed among the overall youth population, the percentage of LGB youth reporting a suicide attempt in the 2019 YRBS is highest among those who identify as more than one race (30.7%), followed by Black youth (27.2%). The percentage is lowest among Asian (21.5%) and White youth (22.3%). Due to the limited number of American Indian and Alaska Native (AI/AN) youth participating in the 2019 YRBS, no national estimate can be reliably calculated for LGB youth who identify as AI/AN. However, in a large national survey of LGBTQ youth conducted by the Trevor Project in 2021, the percentage of youth reporting a suicide attempt was highest among AI/AN youth (31%), which is similar to the pattern observed among the total AI/AN youth population in the 2019 YRBS.[7]
Percentage of LGB youth reporting a suicide attempt in the past 12 months, by race/ethnicity
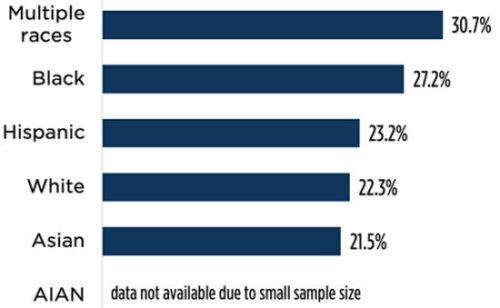
Source: CDC YRBSS (2019)
Suicide risk among LGB youth varies across states.
In 2019, the most recent year for which state-level data from the YRBS are available, approximately 1 in 4 LGB high school students reported a suicide attempt in the past 12 months. However, the percentage ranged from a high of 32.1% in West Virginia to a low of 13.2% in New Jersey, more than a twofold difference.
Currently, few jurisdictions collect data on youth who identify as transgender when administering the YRBS. As a result, it is difficult to examine patterns of risk among transgender youth over time and across states. Given evidence that transgender youth tend to report suicide attempts at higher levels than any other group of youth in the United States, states that do not currently collect data on transgender identity in the YRBS should consider starting.
Percentage of LGB youth reporting a suicide attempt in the past 12 months, national average and states with the lowest and highest percentages.
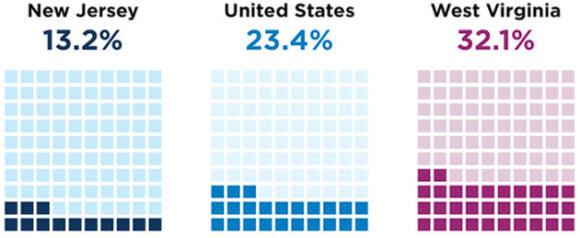
Source: CDC YRBSS (2019)
Suicide Attempts by Race and Ethnicity
Suicide risk is higher among American Indian and Alaska Native youth than their peers.
A larger percentage of youth who identify as AI/AN, Black, or more than one race reported a suicide attempt in the past 12 months than among their Asian, Hispanic, and White peers, according to data from the 2019 YRBS. A similar pattern can be seen in the ABES (2021) data.
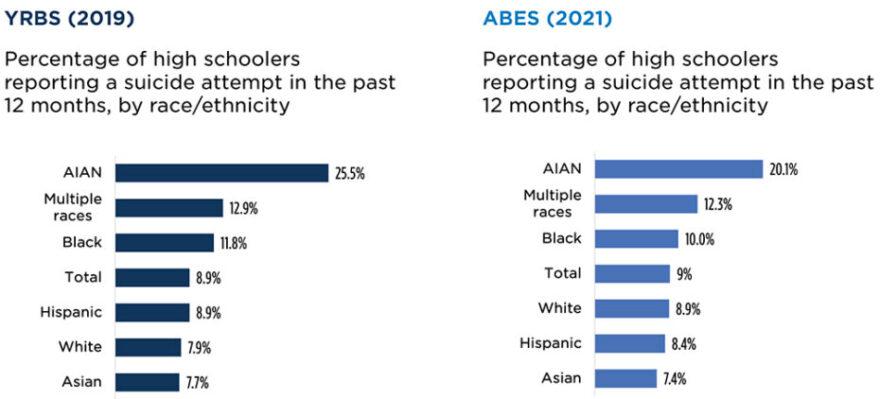
Source: CDC YRBSS (2019); CDC ABES (2021)
Both surveys include a nationally representative sample of youth. However, the ABES was a one- time, online survey while the YRBS is an ongoing paper-and-pencil survey completed in school.
Suicide risk among BIPOC youth varies across states.
The percentage of BIPOC high school students reporting a suicide attempt in the past 12 months varied by state in the 2019 administration of the YRBS. Black females were among the groups with the highest percentage of reported suicide attempts (15.2% vs 11.0% for all females nationwide). However, the percentage ranged from a high of 21.3% in Arkansas to a low of 5.7% in Massachusetts, a nearly four-fold difference. While Hispanic males were the group with the lowest percentage of youth reporting a suicide attempt in the past 12 months nationwide (5.5% vs 6.6% for all males nationwide), the percentage ranged from 24.3% in Alaska to 3.5% in New Jersey, a nearly seven-fold difference.
Percentage of Black female and Hispanic male high school students reporting a suicide attempt in the past 12 months, states with the lowest and highest percentages
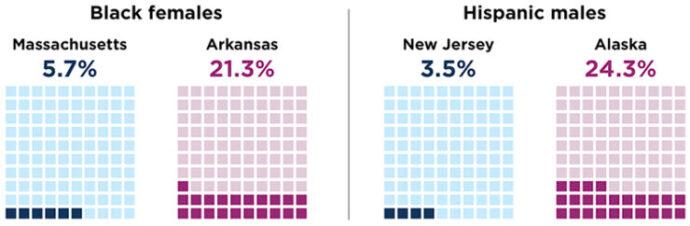
Source: CDC YRBSS (2019)
Suicide Attempts Among Youth With Disabilities
Suicide risk is higher among youth with disabilities.
Relatively limited data are available on suicide risk among youth with disabilities. However, a study published in 2018 found that the percentage of youth with multiple disabilities who reported a suicide attempt in the past 12 months was nearly eight times higher than the percentage of youth with no disabilities who reported a suicide attempt.[8] This pattern aligns with a 2021 study that outlined the ways in which stressors experienced by individuals with disabilities can contribute to their observed higher risk of suicide.[9]
More research is needed to better understand suicide risk among youth with disabilities. Additionally, including disability status on more surveys of adolescent health would allow health and education leaders to better assess their needs and, subsequently, to tailor interventions and track progress in reducing suicide risk among youth with disabilities.
Percentage of youth who reported a suicide attempt in the past 12 months, by disability status
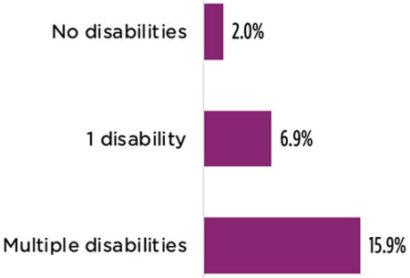
Source: Moses, T. (2018)
Researchers Have Found a Relationship Between Experiences of Discrimination and Suicide Risk
LGBTQ youth
Researchers have found links between discrimination, stigma, and suicide risk among LGBTQ youth. A 2009 study found that perceived discrimination was associated with an increased risk of thoughts of suicide among LGBTQ youth.[10] A study from 2020 found that LGBTQ youth who reported internalized stigma related to their sexual orientation were less likely to say they would seek help if they experienced suicidal thoughts than their LGBTQ peers who did not report internalized stigma.[11] Thus, discrimination and stigma may decrease help-seeking behavior among LGBTQ youth in addition to increasing their risk of suicide thoughts and attempts.
BIPOC youth
Several studies have found a relationship between experiences of racism and risk of suicide, especially among Black youth. A 2017 study found that experiences of discrimination—such as being followed around stores and being called names or insulted—increased the risk of suicidal thoughts among Black youth.[12] A 2022 study found that both overt experiences of racism, such as being harassed or insulted by peers due to one’s race or ethnicity, and subtle experiences of racism— such as feeling that their peers are suspicious of them or don’t listen to them because of their race or ethnicity—were associated with thoughts of suicide among Black and Latinx youth, although the relationship was stronger among Black youth.[13] A 2021 study of American Indian youth living in the Great Plains region found an association between bullying based on race or ethnicity and thoughts of suicide.[14]
Youth with disabilities
Limited research examines the relationship between discrimination and suicide risk among youth with disabilities. A 2018 study found that youth with disabilities were more likely to report suicidal thoughts than their peers without disabilities.[15] Another study from 2021 outlines the evidence for increased risk of suicide among individuals with disabilities and their elevated experiences of marginalization (e.g., social exclusion, prejudice, and discrimination).[16] The author applies minority stress theory,[17] originally developed to describe how the cumulative stressors that LGBTQ individuals experience negatively effects their health, to describe the ways in which stressors experienced by individuals with disabilities can contribute to the observed higher risk of suicide.
Intersectionality
The role of identity-based discrimination in suicide attempts is complex when youth hold multiple marginalized identities. A 2018 study found that peer victimization was a significant predictor of suicidal thoughts among LGBTQ youth and youth with disabilities, and youth who reported high levels of peer victimization and who identified as both LGBTQ and disabled were the most likely to report suicidal thoughts.[18] Another study from 2020 examined the relationship between experiences of discrimination based on sexual orientation and suicide attempts among LGBTQ adults.[19]
They found that this relationship was strongest among young adults (ages 18 to 25) and that the effect of those experiences of discrimination was stronger among Black and Hispanic individuals than their White peers. A 2014 study of suicide among racially diverse LGB youth found that, despite holding more marginalized identities, Asian and Black LGB females had lower risk of suicide than their White counterparts.[20] Ultimately, while more marginalized identities may not always equal more negative outcomes, current evidence highlights the importance of considering the role of identity-based discrimination in suicide risk.
School Connectedness Is a Protective Factor That Reduces Suicide Risk
Research on youth suicide has generally focused more on risk factors than on protective factors. However, a number of studies have identified the importance of protective factors such as school connectedness that reduce youth risk for suicide. In a systematic meta-analysis from 2017, researchers reviewed 16 different studies and found that school connectedness was associated with fewer suicidal thoughts and suicide attempts among all students, but especially among LGBTQ students.[21] A 2018 study found that school connectedness served as a protective factor against suicidal thoughts and attempts for Black youth living in low-income communities.[22]
While school connectedness can serve as a protective factor against suicide, there are documented disparities in school connectedness by race and ethnicity, sexual orientation, and disability status. A 2015 study that examined students in over 400 middle schools found that Black students generally reported lower levels of school connectedness than their White peers.[23] A 2021 study examined school connectedness across different racial, ethnic, sexual orientation, and disability identities and found that females who identify as Black, Asian, Latina, or multiple races had lower levels of school connectedness than their White peers.[24] However, they found the lowest levels of school connectedness among disabled students who also identify as LGBQ, regardless of race.
To better understand the protective role of school connectedness in reducing suicide risk among BIPOC and LGBTQ youth and youth with disabilities, it is important to examine how discrimination can influence school connectedness. A 2020 study found that experiences of racial discrimination—including personal experiences of, witnessing, hearing about, and observing societal forms of discrimination—among a group of Black high school students with elevated disruptive behavior predicted lower school connectedness.[25] The researchers also found that students who perceived their teachers as culturally responsive were more likely to report higher school connectedness, although teacher relationships did not appear to buffer the negative effects of racial discrimination. Overall, protecting LGBTQ youth, Black youth, and youth with disabilities from social discrimination and creating an inclusive environment where these youth feel connected to their schools and peers can serve as a protective factor that reduces suicide risk.
Related Content
- State Policymakers Can Support Equitable School-based Telemental Health Services
- Schools Can Reduce Barriers to Mental Health Access by Ensuring That Services Are Supportive of LGBTQ Youth
- Bridging the Mental Health Care Gap for Black Children Requires a Focus on Racial Equity and Access
- Over One Third of Lower-income Latino Adults Living with Children Have Frequent Anxiety or Depressive Symptoms, and Most Do Not Receive Mental Health Services
A Review of State Suicide Prevention Plans
Most state suicide prevention plans omit the role of discrimination in youth suicide risk.
The Suicide Prevention Resource Center (SPRC) has developed a set of recommendations for state suicide prevention infrastructure that include the development of a plan that is updated every three to five years. The SPRC notes that suicide prevention activities may fall under the responsibility of a number of state-level departments and that state plans can help coordinate efforts more efficiently. Child Trends researchers reviewed state suicide prevention plans archived on the SPRC website in Winter 2021/2022 and found that most state plans overlook the increased suicide risk among BIPOC and LGBTQ adolescents and adolescents with disabilities that results from experiences of discrimination.
Note on methods
State and Territorial Plans Addressing LGBTQ Youth
Twenty-eight state plans describe disparities in suicide risk for LGBTQ youth. Sixteen of those plans reference discrimination faced by LGBTQ youth as a risk factor for suicide. Twenty-four plans omit information specific to LGBTQ youth.
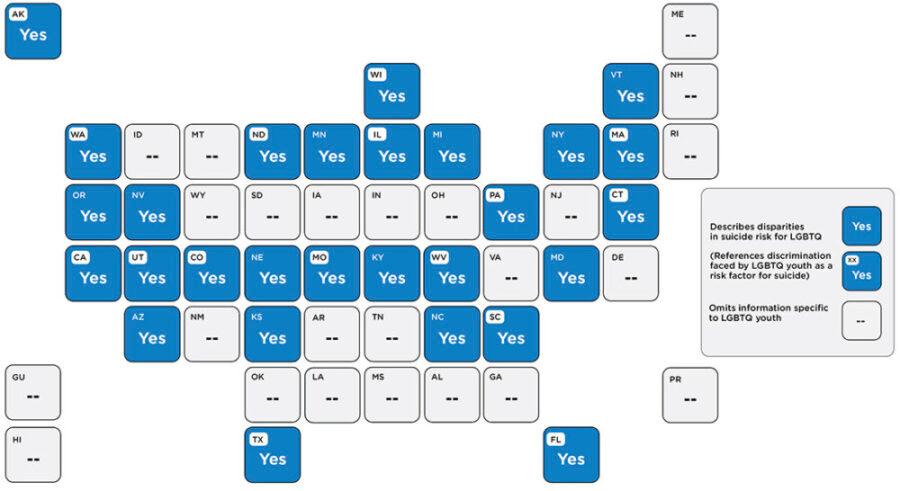
Example from Colorado’s suicide prevention plan addressing the role of discrimination in the risk of suicide for LGBTQ youth
According to the 2019 Healthy Kids Colorado Survey (HKCS), LGBT youth are more likely to experience bullying, feeling unsafe at school, suicidal ideation and attempts, substance use, and sexual violence.
These disparities persist because LGBTQ+ children, youth, and young adults often face discrimination, stigma, and bias, including rejection from family, friends, or community and limited access to LGBTQ+ informed health care.
Children, youth, and young adults who feel supported in their identity (including sexual orientation and gender identity), who have trusted adults in their lives, who feel connected to their school, community and peers, and who have access to culturally competent care are less likely to engage in suicidal behavior, substance use, bullying, and other types of violence and risky behavior.
State and Territorial Plans Addressing BIPOC Youth
Thirty-two plans describe disparities in suicide risk by race. Fourteen of those plans reference racism as a risk factor for suicide. Twenty plans omit information about disparities by race.
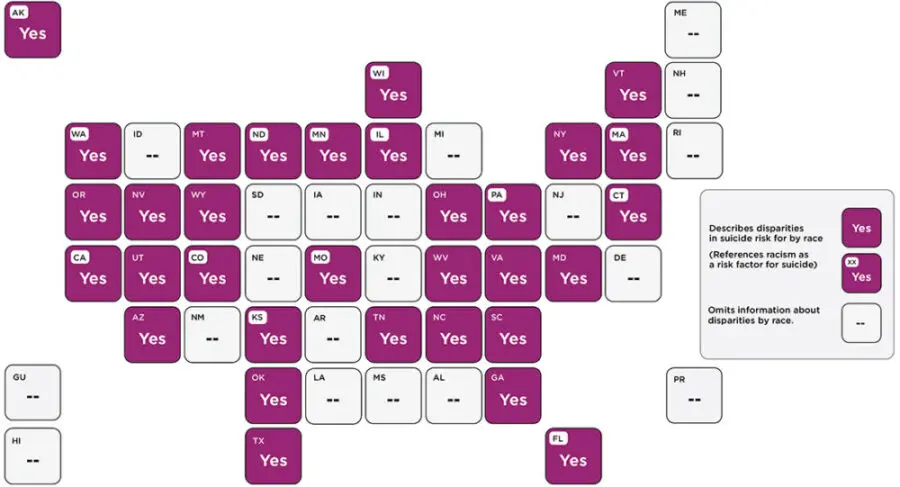
Example from a state suicide prevention plan that addresses the role of racism in the risk of suicide for Alaska Native youth
Historical trauma that has not been adequately acknowledged, expressed, or ultimately resolved, can manifest itself as intergenerational grief that can result in myriad emotional and psychological hardships. It is time for Alaskans to publicly acknowledge the reality of historical trauma and work towards healing. It is also important to note that many Alaska Native communities have important reservoirs of resilience and strength in their traditional values and elders. The suicide rate for Native elders is below the national average.
State and Territorial Plans Addressing Youth With Disabilities
Twelve plans reference discrimination related to disability status, but only five mention the relationship between discrimination and stigma related to disability status and suicide risk. Forty plans omit information specific to disability status among youth.
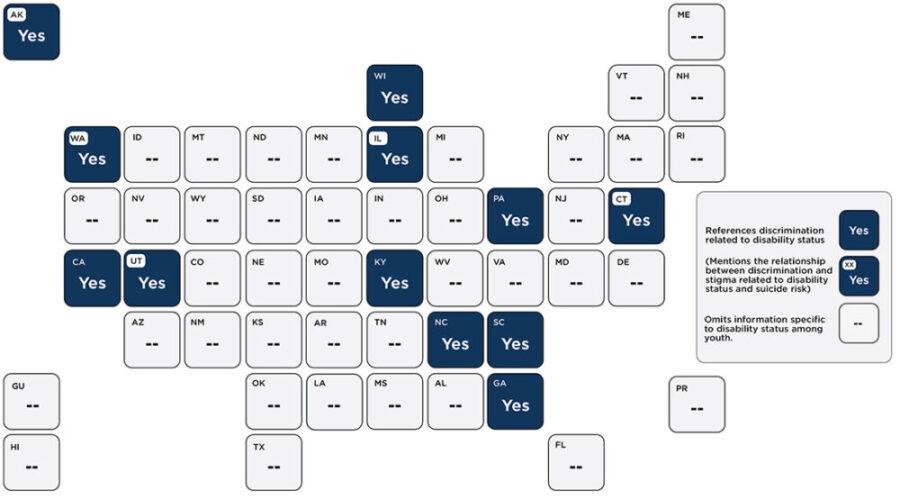
Example from Utah’s suicide prevention plan that addresses the role of discrimination in the risk of suicide for individuals with disabilities
“We can reduce the presence of risk factors, buffer the effects of risk, and empower individuals and communities to be resilient. For example, imagine a middle aged man who was born with a genetic predisposition to depression, who was abused by an overwhelmed parent, who experienced discrimination and temporary school failure due to a disability, and now is geographically isolated and cannot afford to access behavioral health treatment on a consistent basis. Now imagine that this same man had access to academic services and school based social emotional learning programs starting at a young age, had a teacher who believed in his potential, received first generation college financial assistance, has been a long-term member of a community basketball team, has participated in supported employment programs, and occasionally utilizes local support groups and trained clergy supports. This example shows how societal and community supports can dramatically buffer risk factors and change the trajectory of a life.”
Source: https://dsamh-training.utah.gov/_documents/SuicidePrevention/UtahSuicide
PreventionPlan_22-26.pdf
Strategies For State Leaders to Help Ensure That State Suicide Prevention Plans Address Discrimination
1. Ensure that your state’s plan is current.
The COVID-19 pandemic has impacted the physical and mental health of youth and families across the United States. State suicide prevention plans that have not been updated since 2020 may not adequately reflect current risk and protective factors.
2. Collect data on suicide risk that include key demographic characteristics.
The pandemic has highlighted—and in many cases widened—health disparities. Ensuring that data collection includes key demographic characteristics will allow state and local leaders to determine which communities have the greatest need. Such data are also critical for monitoring efforts to reduce disparities in suicide.
3. Call attention to disparities in suicide risk, including by race, sexual orientation, and disability status.
Suicide risk is not evenly distributed. State plans that call attention to disparities can better direct efforts to communities with the greatest need.
4. When discussing disparities in suicide risk, highlight the role of discrimination.
Youth of color, LGBTQ+ youth, and youth with disabilities often experience unique forms of discrimination that place them at higher risk for suicide. State suicide prevention plans that address discrimination can better highlight opportunities to address upstream factors that contribute to well-documented disparities in suicide risk.
5. Emphasize the protective effect of school connectedness.
School connectedness is a protective factor for suicide risk. Several interventions to enhance positive school connections have been found to reduce experiences of victimization and suicide risk. State plans can draw attention to the important role that schools play in reducing experiences of discrimination that contribute to disparities in suicide risk for youth with marginalized identities.
Resources
Below are links to several resources that can equip state leaders with data on suicide risk disparities and best practices for preventing youth suicide, followed by tables with data on suicide attempts per state by race, ethnicity, and sexual orientation.
Youth Risk Behavior Survey (YRBS)
This site allows you to examine trends in youth risk behaviors. Data can be sorted by several characteristics including race, sex, and sexual orientation. Data are also available across multiple years.
Web-based Injury Statistics Query and Reporting System (WISQARS)
This site allows users to examine trends in mortality. Data can be sorted by several characteristics, including race, ethnicity, age, and sex. Data are also available across multiple years.
Suicide Prevention Resource Center
This is a technical assistance center funded by SAMHSA. The site has several resources, including an archive of state suicide prevention plans and guidance on implementing a comprehensive approach that promotes connectedness.
CDC Division of Adolescent and School Health
This webpage is hosted by CDC DASH and includes several resources related to school connectedness. Resources include practical guidance for equipping schools to promote positive connections, such as guidance targeting school districts, school leaders, school staff, and families.
Appendix 1: Percentage of Youth Reporting Suicide Attempt per State, by Sexual Orientation (YRBS, 2019)
Appendix 2: Percentage of Youth Reporting Suicide Attempt per State, by Race & Ethnicity (YRBS, 2019)
Stratford, B., Surani, K., Gabriel, A., & Abdi, F. (2022). Addressing discrimination supports youth suicide prevention efforts. Child Trends. https://doi.org/10.56417/3349i4871b
Footnotes
[1] 1 CDC Web-based Injury Statistics Query and Reporting System
[2] CDC ABES
[3] Moses, T. (2018). Suicide attempts among adolescents with self-reported disabilities. Child Psychiatry & HumanDevelopment, 49(3), 420-433.
[4] Johns, M. M., Lowry, R., Andrzejewski, J., Barrios, L. C., Demissie, Z., McManus, T.,… & Underwood, J. M. (2019). Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. Morbidity and Mortality Weekly Report, 68(3), 67.
[5] King, M. T., Merrin, G. J., Espelage, D. L., Grant, N. J., & Bub, K. L. (2018). Suicidality and intersectionality among students identifying as nonheterosexual and with a disability. Exceptional Children, 84(2), 141-158.
[6] Johns, M. M., Lowry, R., Andrzejewski, J., Barrios, L. C., Demissie, Z., McManus, T., … & Underwood, J.M. (2019). Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. Morbidity and Mortality Weekly Report, 68(3), 67.
[7] The Trevor Project. (2021). 2021 National Survey on LGBTQ Youth Mental Health. West Hollywood, California: The Trevor Project.
[8] Moses, T. (2018). Suicide attempts among adolescents with self-reported disabilities. Child Psychiatry & Human Development, 49(3), 420-433.
[9] Lund, E. M. (2021). Examining the potential applicability of the minority stress model for explaining suicidality in individuals with disabilities. Rehabilitation Psychology, 66(2), 183–191
[10] Almeida, J., Johnson, R. M., Corliss, H. L., Molnar, B. E., & Azrael, D. (2009). Emotional distress among LGBT youth: The influence of perceived discrimination based on sexual orientation. Journal of youth and adolescence, 38(7), 1001-1014.
[11] Chang, C. J., Kellerman, J., Feinstein, B. A., Selby, E. A., & Goldbach, J. T. (2020). Greater minority stress is associated with lower intentions to disclose suicidal thoughts among LGBTQ+ youth. Archives of suicide research, 1-15.
[12] Assari, S., Moghani Lankarani, M., & Caldwell, C. H. (2017). Discrimination increases suicidal ideation in black adolescents regardless of ethnicity and gender. Behavioral sciences, 7(4), 75.
[13] Madubata, I., Spivey, L. A., Alvarez, G. M., Neblett, E. W., & Prinstein, M. J. (2022). Forms of Racial/Ethnic Discrimination and Suicidal Ideation: A Prospective Examination of African-American and Latinx Youth. Journal of Clinical Child & Adolescent Psychology, 51(1), 23-31.
[14] Edwards, K. M., Banyard, V. L., Charge, L. L., Kollar, L. M. M., & Fortson, B. (2021). Experiences and correlates of violence Among American Indian and Alaska Native youth: a brief report. Journal of interpersonal violence, 36(23-24), 11808-11821.
[15] King, M. T., Merrin, G. J., Espelage, D. L., Grant, N. J., & Bub, K. L. (2018). Suicidality and intersectionality among students identifying as nonheterosexual and with a disability. Exceptional Children, 84(2), 141-158.
[16] Lund, E. M. (2021). Examining the potential applicability of the minority stress model for explaining suicidality in individuals with disabilities. Rehabilitation Psychology, 66(2), 183–191.
[17] Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological bulletin, 129(5), 674.
[18] King, M. T., Merrin, G. J., Espelage, D. L., Grant, N. J., & Bub, K. L. (2018). Suicidality and intersectionality among students identifying as nonheterosexual and with a disability. Exceptional Children, 84(2), 141-158.
[19] Layland, E. K., Exten, C., Mallory, A. B., Williams, N. D., & Fish, J. N. (2020). Suicide attempt rates and associations with discrimination are greatest in early adulthood for sexual minority adults across diverse racial and ethnic groups. LGBT health, 7(8), 439-447.
[20] Bostwick, W. B., Meyer, I., Aranda, F., Russell, S., Hughes, T., Birkett, M., & Mustanski, B. (2014). Mental health and suicidality among racially/ethnically diverse sexual minority youths. American journal of public health, 104(6), 1129-1136.
[21] Marraccini, M. E., & Brier, Z. M. (2017). School connectedness and suicidal thoughts and behaviors: A systematic metaanalysis. School psychology quarterly, 32(1), 5.
[22] Tomek, S., Burton, S., Hooper, L. M., Bolland, A., & Bolland, J. (2018). Suicidality in Black American youth living in impoverished neighborhoods: Is school connectedness a protective factor?. School mental health, 10(1), 1-11.
[23] Voight, A., Hanson, T., O’Malley, M., & Adekanye, L. (2015). The racial school climate gap: Within-school disparities in students’ experiences of safety, support, and connectedness. American journal of community psychology, 56(3), 252-267.
[24] Forber-Pratt, A. J., Merrin, G. J., & Espelage, D. L. (2021). Exploring the intersections of disability, race, and gender on student outcomes in high school. Remedial and Special Education, 42(5), 290-303.
[25] Bottiani, J. H., McDaniel, H. L., Henderson, L., Castillo, J. E., & Bradshaw, C. P. (2020). Buffering effects of racial discrimination on school engagement: The role of culturally responsive teachers and caring school police. Journal of School Health, 90(12), 1019-1029.
This brief is supported by cooperative agreement NU87PS004367-01-01 funded by the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views or endorsement of the CDC or the Department of Health and Human Services.
Download
© Copyright 2025 ChildTrendsPrivacy Statement
Newsletter SignupLinkedInYouTubeBlueskyInstagram