

Reducing teen pregnancy rates in the United State—a factor that influences birth rates—has been a federal program priority for several decades; since peaking in the early 1990s, birth rates among adolescents ages 15 to 19 have declined substantially. While numerous studies of early childbearing have identified lower socioeconomic attainment for parents and poorer developmental outcomes for children, the long-term health and socioeconomic effects of early childbearing for parents are also a concern and have not been assessed.
Despite declines over the last three decades, nearly 172,000 teens had a child in 2019, and the historical and social contexts that have contributed to persistent disparities in teen birth outcomes cannot be ignored. Within the United States, teen birth rates vary greatly by demographics, including race, ethnicity, and geography (region, state, county, and urban vs. rural). Social determinants of health, including family education and income levels and community- or neighborhood-level socioeconomic factors—as well as differences in adolescents’ access to high-quality sexual and reproductive health services—can also contribute to high teen birth rates.
In this brief, we describe the results of our simulation of the effects of preventing births to teenagers on the teens’ long-term well-being. That is, for youth who had a child by age 19, we estimated what their long-term outcomes would have been if they had not had a child as a teen. (Our simulation employed the Social Genome Model; read more about this model below.) We find positive effects on education, physical and mental health, earnings, poverty, and lifetime income when births to teens are prevented.
About the Social Genome Model
The Social Genome Model is a microsimulation tool that allows us to project how changes that take place earlier in someone’s life course (e.g., during adolescence) reverberate through an adolescent’s life into adulthood without having to wait decades for longitudinal real-world data from programs or intervention evaluations focused on reducing the teen birth rate. Through the use of a Social Genome Model simulation, we can project how adolescents’ outcomes may have been different later in life if they had not had a child by age 19.
Learn more about the Social Genome Model, a partnership between Child Trends, the Brookings Institution, and the Urban Institute.
Our Research Approach
To project how later life outcomes might change if teens did not have a child during adolescence, we reduced the probability of having a child for all Social Genome Model respondents who were likely to have a child by age 19 to zero (approximately 17% of the Social Genome Model population). We then observed how this change might affect outcomes at all subsequent life stages.
Learn more about the Social Genome Model’s measure of teen birth that was used in this model.
At the transition to adulthood (age 24), we examine educational attainment, mental and physical health, and the income-to-poverty ratio. At adulthood (age 30), we describe bachelor’s degree attainment and earnings. We also project lifetime earnings through age 65, based on individuals’ education and earnings at age 30. Since young mothers are more likely to raise children, we examine differences by sex of the teen parent. We also examine differences by race given disparities in teen birth rates by race and ethnicity. All outcomes are estimated net of the variables included in previous life stages.
Note: For all figures and tables in this brief, the White and other race group includes a small percentage of people who identify as Native American, Asian or Pacific Islander, or more than one race; because of sample size constraints, the Social Genome Model cannot estimate simulations separately for this group.
Findings From a Simulation of Preventing Teen Births
Our simulation results indicate that, among young people who had births during their teen years, several outcomes in adulthood would have been improved if those births had been prevented. The tables below show the results of the simulation overall and for each racial/ethnic and sex group.
Health, education, and poverty outcomes are better in early adulthood (age 24) when teen births are prevented.
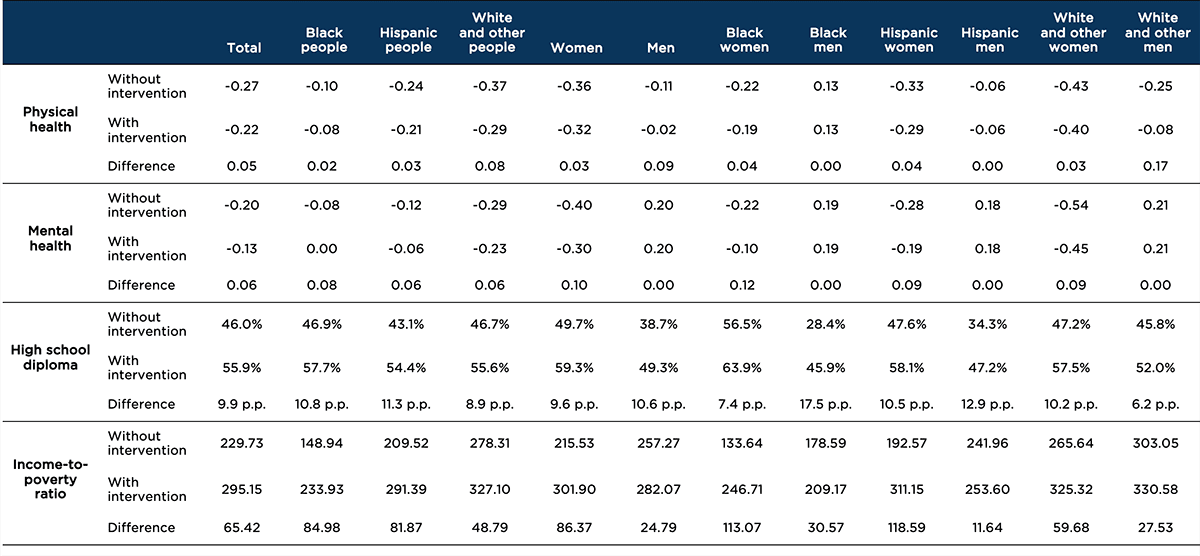
We found that preventing teenage births results in improvements in high school completion, physical and mental health, and poverty status. Table 2 shows these outcomes in the transition to adulthood (age 24) if an adolescent had a child by age 19 (“Without intervention”) and what their outcomes would be if the birth were prevented (“With intervention”).
At age 24, there are notable improvements to physical and mental health, particularly the mental health of women overall—and most especially Black women. High school diploma attainment increases by at least 6 percentage points (for White males) and up to 18 percentage points (for Black males). And, by age 24, household incomes increase substantially relative to the poverty level, particularly for young women. The income-to-poverty ratio reflects both earnings and the number of people dependent on earnings: The rather substantial improvements shown in the table that result from preventing teenage births are likely due to both greater earnings for young people and fewer dependents.
Table 2. Simulated transition to adulthood (age 24) outcomes resulting from preventing teen births, by race/ethnicity and sex
Notes: n = 68,720.
Educational outcomes are the percentage of people who receive the degree, and the difference is expressed in percentage points (p.p.). Mental health and physical health outcomes are standardized and units are standard deviations; thus, a negative “Without intervention” score indicates that the average score was below the mean. The income-to-poverty ratio is a continuous measure. The “Difference” row in the table reports the magnitude of the change in outcome for each of the six race/ethnicity/sex groups. The White and other race group includes a small percentage of people who identify as Native American, Asian or Pacific Islander, or more than one race; because of sample size constraints, the Social Genome Model cannot estimate simulations separately for this group.
Source: Social Genome Model
College degrees and earnings are higher at age 30 when teen births are prevented.
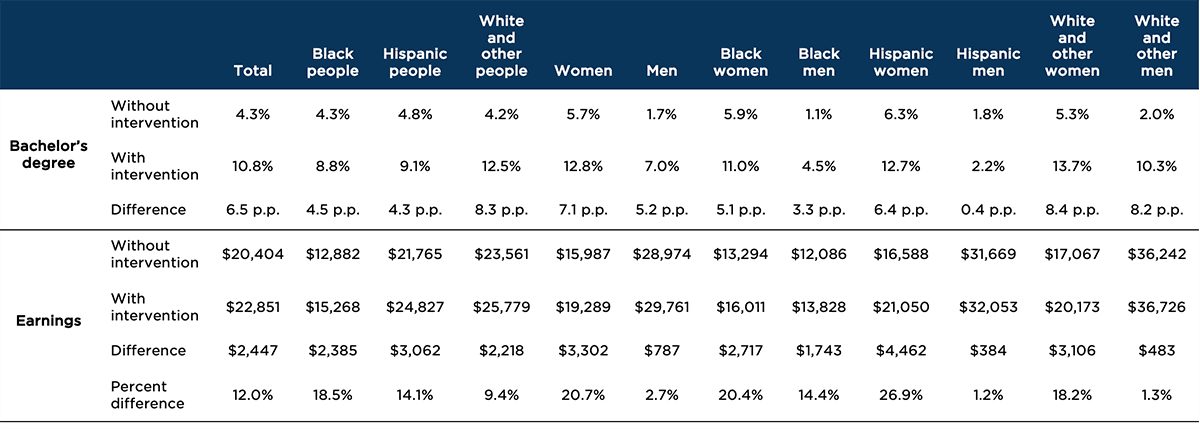
Our simulation indicates that preventing teen births is also associated with increases in bachelor’s degree attainment and annual earnings at age 30. Our analysis (see Table 3) finds notable increases in attainment of a bachelor’s degree by age 30, with increases of 3 to 8 percentage points—with the exception of Hispanic men, who experience no change in these outcomes from preventing teen births. By age 30, bachelor’s degree attainment increases by about 5 percentage points for men and 7 percentage points for women. White and other men and women have the greatest educational gains, by 8 percentage points. Hispanic women and Black women have large gains as well, with 6 and 5 percentage point increases, respectively.
The simulation also indicates increases in age 30 annual earnings by $384 (to $4,462) when births are prevented. Women overall had a substantially larger income increase than men. Among women, Hispanic women had the greatest increase with $4,462, followed by White and other women ($3,106) and Black women ($2,717).
Table 3. Simulated increase in bachelor’s degree attainment and earnings at age 30 resulting from preventing teen births, by race/ethnicity and sex
Notes: n = 68,720.
Educational outcomes are the percentage of people who received the degree, and the difference is expressed in percentage points (p.p.). Earnings are the respondent’s total income from wages or salary, adjusted for inflation. The “Difference” row in the table reports the magnitude of the change in outcome for each of the six race/ethnicity/sex groups. The White and other race group includes a small percentage of people who identify as Native American, Asian or Pacific Islander, or more than one race; because of sample size constraints, the Social Genome Model cannot estimate simulations separately for this group.
Source: Social Genome Model
Lifetime earnings also increase when teen births are prevented.
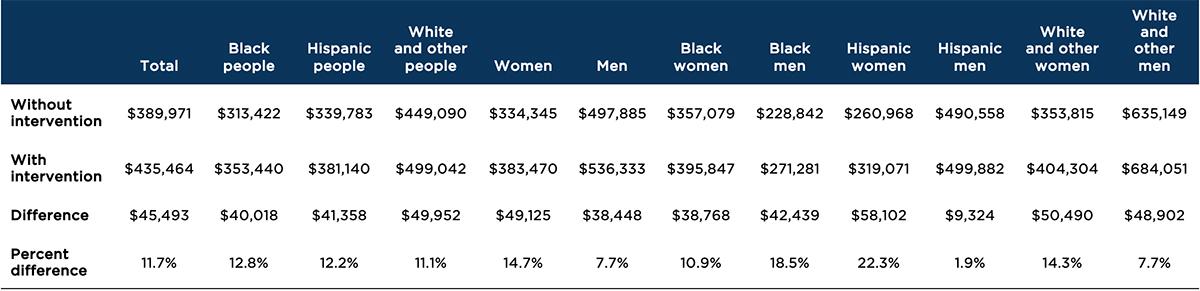
We also found increases in lifetime earnings as a result of preventing teen births. These patterns are similar to those found for age 30 earnings, with Hispanic women seeing the greatest increase in both dollar earnings ($58,102) and percent increase (22%). Although White and other women have the next highest dollar increase ($50,490; a 14% increase), Black males also experience a substantial percentage increase ($42,439; a 19% increase). Overall, lifetime earnings at age 65 increase by an average of $49,125 for women and $38,448 for men.
Table 4. Simulated lifetime (age 65) earnings resulting from preventing teen births, by race/ethnicity and sex
Notes: n = 68,720.
Lifetime earnings are discounted present values in 2018 dollars; undiscounted lifetime earnings would be about twice as much. The “Difference” row in the table reports the magnitude of the change in outcome for each of the six race/ethnicity/sex groups. The White and other race group includes a small percentage of people who identify as Native American, Asian or Pacific Islander, or more than one race; because of sample size constraints, the Social Genome Model cannot estimate simulations separately for this group.
Source: Social Genome Model
Discussion
Our simulation using the Social Genome Model indicates that preventing teen births is associated with important differences in life outcomes for everyone, but especially for women. When teen births are prevented in this simulation, young women attain more years of education, have higher earnings, experience higher incomes relative to the poverty level, and enjoy better mental health. These analyses suggest that early childbearing continues to be associated with long-term negative education and economic implications. One potential complicating factor: Since teen parents tend to enter the labor market at younger ages, by age 30 they have had more time to acquire job experience and salary increases. Thus, economic effects may be less apparent at age 30 than they will be later in life. Indeed, our simulation of lifelong earnings (age 65) shows substantial long-term gains in earnings when a teen birth is prevented.
These findings also have implications for equity. While rates of early childbearing have declined dramatically among Black, Hispanic, and White teens, rates remain higher among youth of color. These differences likely reflect structural impediments, including inequitable access to positive opportunities for education and career advancement, disparities in the availability and provision of medically accurate information on sexual and reproductive health, and disparities in knowledge of and access to contraceptive and other reproductive health services; together, these factors can limit educational and economic mobility. Furthermore, the lack of resources to support young parents as they continue their education—such as low availability of publicly funded family planning services or on-campus child care—can also contribute to continued disparities and repeat births. Given these relationships, policies, programs, and other prevention efforts must be more intentional in meeting the needs of young people in these communities.
Limitations
As with all microsimulations, this study has limitations that users should consider when interpreting its findings. First, the Social Genome Model is not a causal model and cannot be used to make causal conclusions; therefore, our simulation should be considered as a potential scenario. Second, all regressions underlying the model are linear—the model does not account for any path that can lead to quadratic or cubic effects, nor does it account for any non-linear path. Third, the longitudinal data used in our model are older by design in order to have data through age 30 (NLSY97 respondents were born during the years 1980 through 1984), and the Social Genome Model dataset may not fully represent the characteristics of adolescents today. Also, all benefits of the simulation are quantified for individuals—not for society. The results presented in this brief do not encompass the benefits to society that are associated with having a better-educated, healthier, and higher-earning population. Lastly, because these results focus on outcomes for parents, they do not assess outcomes for children. Substantial research has found negative effects of poverty, family instability, and other adverse childhood experiences on the development of children, all of which are more common among young parents.
In addition, while we are able to stratify our simulations by race/ethnicity (Black, Hispanic, and White and other) and by sex (male and female)—to account for underlying social and economic differences and to identify the different effects that preventing teen births would have for each group—we’re unable to account for all of the heterogeneity in teen birth experiences. The Social Genome Model measure of having a child(ren) by adolescence (before age 20) groups all adolescent experiences together and is unable to assess differences in outcomes that could result if the adolescent were an older teen when they had their child(ren) or if the pregnancy were wanted. The Social Genome Model also does not include measures of protective factors or supports from which adolescents in our sample might benefit (e.g., adolescent is married; adolescent was a high school graduate before they had their child; family, friends, or adolescents’ school or workplace provide child care), and which would mitigate the potential consequences of having a child(ren) during the teen years. Finally, this simulation does not directly account for social determinants of health—such as racial segregation, income inequality, access to health care and health insurance, and the type and receipt of school-based sexual education—that may contribute to higher teen birth rates.
Considerations for future research and programs
Research and programmatic efforts should continue to encourage and support teens in delaying childbearing. While some births, especially to older teens, are desired, most teen births are not. Moreover, relationships initiated at young ages are highly likely to break up, undermining the economic and social support available to the parent and to the child. Our simulation results using the Social Genome Model indicate that important increases in education, earnings, mental health, and income relative to poverty would occur for young people of color, especially, as teen births are averted.
Research has concluded that simply providing information on abstinence and contraceptive methods does not yield significant changes in youth sexual behaviors. Instead, evidence suggests that comprehensive sexuality education and taking a positive youth development approach to adolescent sexual and reproductive health may be more effective. Examples of potentially successful prevention efforts include encouraging educational engagement, implementing evidence-based teen pregnancy prevention programs, providing medically accurate information about reproductive health and contraception, improving access and utilization of teen-friendly health services and school-based sexual and reproductive health services, expanding access to family planning services and Title X clinics, and integrating positive youth development and a social determinants of health approach into teen pregnancy prevention.
One example of a research-based sexual health promotion program that is grounded in positive youth development principles is El Camino, a curriculum developed by Child Trends. This free curriculum, available in both English and Spanish, encourages adolescents to articulate their personal goals and identify strategies to reach their goals, allowing them to assess whether early parenthood aligns with the goals they identified. When adolescents consider the effects of childbearing on their lives and personal goals, many become more open to information and messages about practicing safe sex and delaying sex and pregnancy.
Despite the best research and programmatic investments in and attention on preventive efforts, we know that teen births will continue to occur. It is important that we also invest in navigation services and programs and resources that will support and meet the diverse needs of expectant and parenting teens so that all teens (and their children) have the opportunity to thrive.
While the rate of teen childbearing has declined in the United States, rates remain considerably higher than in other developed nations. The experiences of other countries suggest that continued reductions in the frequency of adolescent parenthood are possible. Our Social Genome Model simulation suggests that delays in teen parenthood would yield substantial benefits for young people across racial and ethnic groups.
Suggested citation
McClay, A., & Moore, K.A. (2022). Preventing births to teens is associated with long-term health and socioeconomic benefits, according to simulation. Child Trends. https://doi.org/10.56417/2270z3088p
Acknowledgements
The authors would like to thank Asari Offiong for her expert review and substantive feedback on this product, Katelyn Rust for their thorough fact check, and the Child Trends communications team for product design and dissemination. We also thank Gabriel Piña and Vanessa Sacks for their thought partnership and methodological review of this simulation design, as well as their collaboration on the Social Genome Model project.
© Copyright 2025 ChildTrendsPrivacy Statement
Newsletter SignupLinkedInYouTubeBlueskyInstagram