

Children who are exposed to traumatic life events are at significant risk for developing serious and long-lasting problems across multiple areas of development.[1],[2],[3],[4] However, children are far more likely to exhibit resilience to childhood trauma when child-serving programs, institutions, and service systems understand the impact of childhood trauma, share common ways to talk and think about trauma, and thoroughly integrate effective practices and policies to address it—an approach often referred to as trauma-informed care (TIC).[5]
TIC is not the sole responsibility or purview of mental health professionals. While evidence-based trauma treatment can play a significant role in the healing process for children who need it, there are many other ways to implement TIC. In fact, every program and service system that touches the lives of children can play an important role.
This brief summarizes current research and promising practices for implementing TIC to support the well-being of children exposed to trauma and help them reach their full potential. The brief begins with an overview of the nature, prevalence, and impact of childhood trauma, followed by a discussion of related risk factors associated with poor child outcomes and protective factors that support resilience. In addition, we present a framework for understanding and implementing trauma-informed care in programs and service systems for children and their families.
Childhood trauma
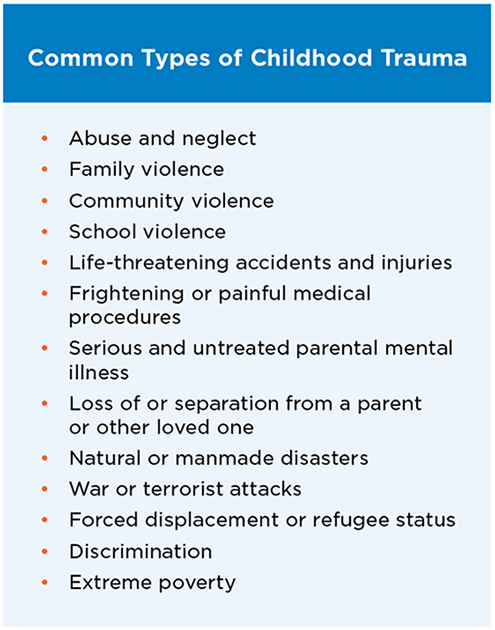
Childhood trauma occurs when a child experiences an actual or threatened negative event, series of events, or set of circumstances that cause emotional pain and overwhelm the child’s ability to cope.[6],[7],[8] Childhood trauma is widespread and can take many forms (see Figure 1 for common types of childhood trauma).[9],[10]
Trauma exposure often begins early in life. Young children are at the highest risk for exposure to trauma and are most vulnerable to its adverse effects.[11] An estimated half of all children in the United States—approximately 35 million—are exposed to at least one type of trauma prior to their eighth birthday.[12] For example, child abuse and neglect are most common among children younger than age 3.[13] Children under age 5 are most likely to incur injuries from falls, choking, and poisoning,[14] and represent the majority of children who witness domestic violence.[15] Children from certain racial and ethnic groups also are more likely to experience adversities that can cause trauma. For example, exposure to childhood adversity is more common among black and Hispanic children than among white children, even when accounting for the role of income.[16]
Impact of childhood trauma
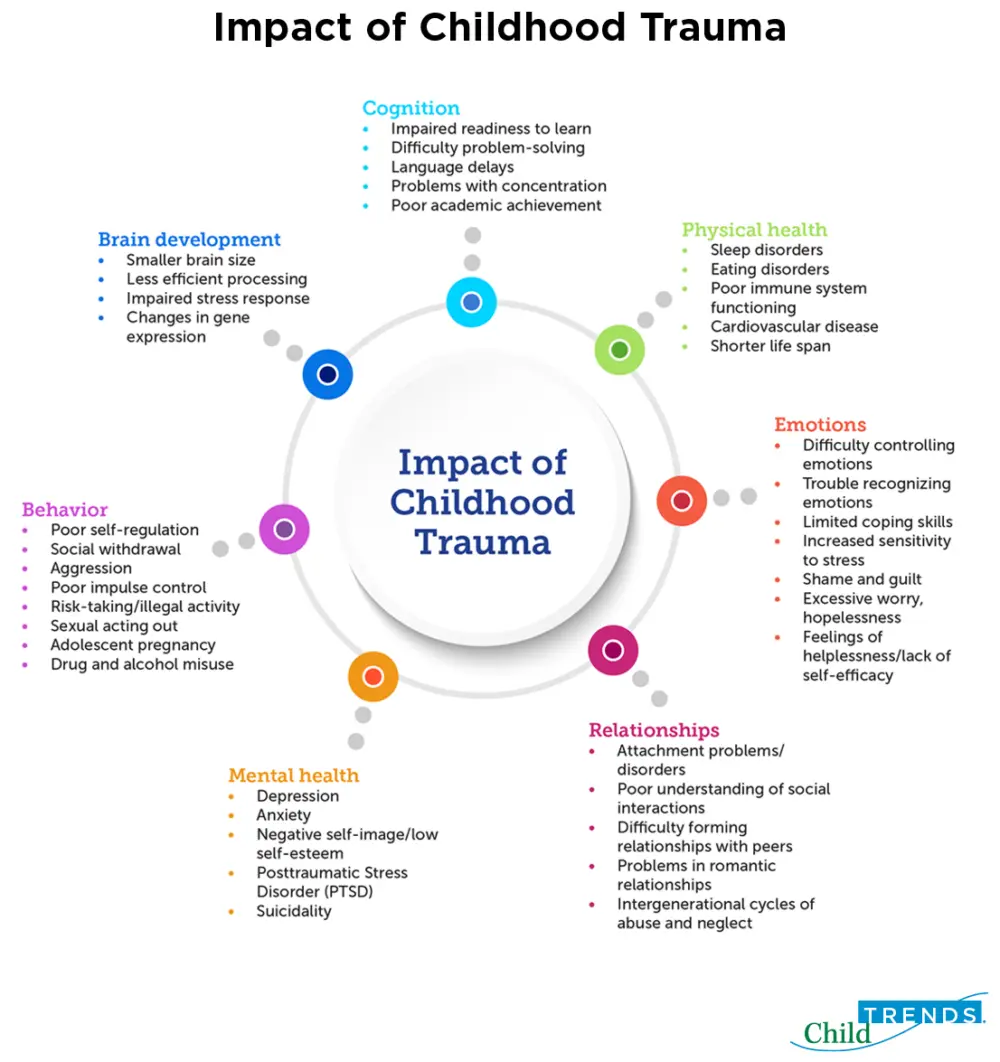
Childhood trauma is strongly linked to mental and physical health problems over the lifespan. It negatively impacts brain development, cognitive development, learning, social-emotional development, the ability to develop secure attachments to others, and physical health; it is also associated with a shortened lifespan[17],[18],[19],[20] (see Figure 2 for additional information on the impact of childhood trauma). A considerable body of research demonstrates that children suffer the most severe, long-lasting, and harmful effects when trauma exposure begins early in life, takes multiple forms, is severe and pervasive, and involves harm by a parent or other primary caregiver—often referred to as complex trauma.[21]
Childhood trauma is more likely to lead to post-traumatic stress disorder (PTSD) than trauma that occurs in adulthood.[22] Children exposed to several different forms of trauma are more likely to exhibit PTSD (e.g., anxiety, depression, anger, aggression, dissociation) than children with chronic exposure to a single type of trauma.[23] Children and youth with PTSD may re-experience the traumatic event through intrusive memories, nightmares, and flashbacks; avoid situations or people that remind them of the trauma; and feel intense anxiety that disrupts their everyday lives. In addition, they may engage in aggressive, self-destructive, or reckless behavior; have trouble sleeping; or remain in a state of hypervigilance, an exaggerated state of awareness and reactivity to their environments.[24] However, there is no typical reaction to trauma. The vast majority of children show distress immediately following a traumatic event, but most return to their prior level of functioning.[25]
Generally, children’s reactions to trauma differ based on the nature of the trauma; the child’s individual, family, and neighborhood characteristics; and the overall balance of risk and protective factors in their lives. It also depends on their age and developmental stage.[26],[27]
Young children who experience trauma may:
- Have difficulties forming an attachment to caregivers
- Experience excessive fear of strangers or separation anxiety
- Have trouble eating and sleeping
- Be especially fussy
- Show regression after reaching a developmental milestone (e.g., sleeping through the night, toilet training)
School-age children who experience trauma may:
- Engage in aggressive behavior
- Become withdrawn
- Fixate on their own safety or the safety of others
- Re-enact the traumatic event through play
- Have frequent nightmares
- Exhibit difficulty concentrating in school
Adolescents who experience trauma may:
- Become anxious or depressed
- Engage in risk-taking or self-destructive behaviors (e.g., drug and alcohol misuse, dangerous driving, sexual promiscuity, unprotected sex, self-harm, illegal activity)
- Feel intense guilt, anger, or shame
- Adopt a negative view of people and society
- In some cases, have persistent thoughts about suicide or seeking revenge
Resilience to Childhood Trauma
When parents, service providers, and programs employ a resilience framework to childhood trauma, they understand there are always opportunities to support positive developmental trajectories among children, even if they have experienced trauma. Resilience has been defined as “a dynamic process encompassing positive adaptation within the context of significant adversity.”[28] Resilience is not a personal trait that individuals do or do not possess (thus, the term “resiliency” is best avoided because it connotes an individual characteristic),[29] but rather a product of interacting factors—biological, psychological, social, and cultural—that determine how a child responds to traumatic events.[30]
Resilience to trauma can be defined in several ways: positive child outcomes despite exposure to trauma, prevention of trauma recurrence despite high risk for further exposure, or avoidance of traumatic experiences altogether in the face of significant risk. All three of these conceptualizations of resilience are based on an ecological approach.
Ecological approach to resilience. Using an ecological approach to promote resilience in development among children who experience trauma is useful because it assumes that there are multiple levels of influence on a child’s development—the individual, parent, family, school, community, and culture—which may increase or decrease a child’s risk for and response to experiencing trauma. These various influences are often referred to as risk and protective factors.[31]
Risk factors. Risk factors are circumstances, characteristics, conditions, events, or traits at the individual, family, community, or cultural level that may increase the likelihood a person will experience adversity (e.g., childhood trauma, re-traumatization, or negative outcomes due to trauma).[32],[33] Risk factors for specific types of trauma may vary, but commonly include living in poverty, a lack of social supports, and prior history of trauma.[34],[35] Additionally, children who identify as lesbian, gay, bisexual, transgender, or queer (LGBTQ)[36] and children in military families[37] are at an increased risk for experiencing trauma. However, the presence of risk factors or membership in a high-risk group does not necessarily mean that a child will experience trauma or its most adverse effects.[38] Protective factors can buffer children from risk and improve the odds of resilient functioning.
Protective factors. Protective factors are characteristics, conditions, or events that promote healthy development and minimize the risk or likelihood a person will experience a particular illness or event, or its related negative outcomes.[39] Research shows that the strongest protective factor linked with resilience to childhood trauma is the reliable presence of a sensitive, nurturing, and responsive adult.[40] The presence of such a figure can help children by restoring a sense of safety, predictability, and control; giving them the feeling of safety; providing them a way to process traumatic events; protecting them from re-traumatization; supporting their development of self-regulation; and helping them heal.[41], [42],[43],[44]
In addition, the National Child Traumatic Stress Network highlights the following protective factors that promote resilience to childhood trauma:[45]
- Support from family, friends, people at school, and members of the community
- A sense of safety at home, at school, and in the community
- High self-esteem and positive sense of self-worth
- Self-efficacy
- Spiritual or cultural beliefs, goals, or dreams for the future that provide a sense of meaning to a child’s life
- A talent or skill in a particular area (e.g., excelling in school or in a sport)
- Coping skills that can be applied to varying situations
Finally, resilience to childhood trauma depends largely on the supports available to a child and his or her family. Family members, teachers, mental health providers, child welfare workers, and other community service providers can work together to ensure that children and families receive the emotional and concrete supports (e.g., food, shelter, financial stability) they need.[46] This system of care approach is also a cornerstone of TIC.[47]
Trauma-informed Care
The context in which children live, learn, and grow shapes both their immediate and long-term well-being.[48] Accordingly, children who experience trauma are more likely to exhibit resilience when their environments are responsive to their specific needs. Families, schools, community-based programs and services, and the individuals caring for children can increase the chances of resilience following childhood trauma when they become aware of the impact of childhood trauma, provide a sense of safety and predictability, protect children from further adversity, and offer pathways for their recovery. In other words, children benefit when these entities provide them with trauma-informed care (TIC).[49]
Implementing TIC with child-serving programs, institutions, and systems
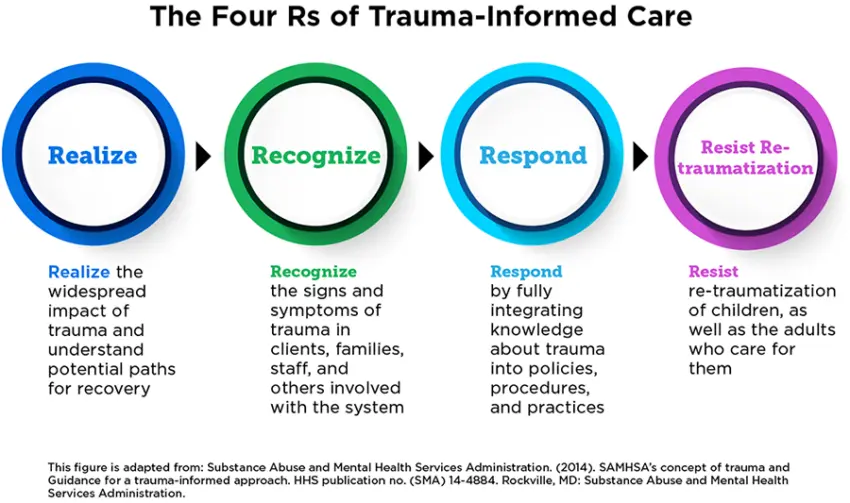
Despite its focus on trauma, TIC is inherently a strengths-based perspective that emphasizes resilience instead of pathology.[50] TIC has been defined and implemented in a number of ways, but the Substance Abuse and Mental Health Services Administration has identified four key elements—the Four Rs (see description of each “R” below)—that can be used broadly across programs, institutions, and services.[51]
Applying TIC to real-world settings begins with a child’s first contact with a program, institution, or service system. It requires a comprehensive and multi-pronged effort involving the many adults in children’s lives. For example, in a school or afterschool program, TIC means increasing trauma-related knowledge and skills among program facilitators, school administrators, bus drivers, food service workers, classroom assistants, administrative staff, volunteers, teachers, leadership, special education professionals, school social workers and psychologists, families, and anyone else who comes into contact with children. However, increasing trauma knowledge is only one aspect of TIC, which also means that the individuals who care for children must be able to:
- Realize the widespread nature of childhood trauma and how it impacts the child’s emotional, social, behavioral, cognitive, brain, and physical development, as well as their mental health. In addition, adults must be aware of the influence of trauma on family members, first responders, service providers, and others who may experience secondary stress (trauma-related reactions to exposure to another person’s traumatic experience).[52],[53] In some instances, adults endure the same traumatic events or circumstances as the child (e.g., a natural disaster, community violence, death of a community member) and may benefit from similar supports.
- Recognize the symptoms of trauma, including how trauma reactions (i.e., symptoms of posttraumatic stress) vary by gender, age, type of trauma, or setting. In addition, the adults in children’s lives must understand that a child’s challenging behaviors are normal, self-protective, and adaptive reactions to highly stressful situations, rather than viewing that child as intentionally misbehaving. Children’s trauma reactions are understood to be adaptive efforts to protect themselves in response to traumatic events. For example, a child may be hypervigilant to an adult’s anger or disapproval because, in the past, he or she experienced physical abuse by a parent. Or, a child may disassociate or daydream as a learned response that enables them to avoid feeling or thinking about a traumatic experience.[54] In addition, TIC means recognizing that trauma may influence a child’s engagement in activities and services, interactions with peers and adults, and responsiveness to rules and guidelines.[55]
- Respond by making necessary adjustments, in their own language and behavior, to the child’s environment; and to policies, procedures, and practices to support the child’s recovery and resilience to trauma.[56]
- Resist re-traumatization by actively shaping children’s environments to avoid triggers (sounds, sights, smells, objects, places, or people that remind an individual of the original trauma) and protect children from further trauma, which can exacerbate the negative impacts of trauma and interfere with the healing process.[57],[58]
Training and professional development on child trauma is an important first step in TIC. Providing adults (staff, leadership, families, and community partners) with training and professional development on childhood trauma is an important component of implementing TIC.[59] It is essential that adults become aware of the prevalence and impact of trauma, and learn to apply a “trauma lens” (i.e., gain the capacity to view children’s difficulties in behavior, learning, and relationships as natural reactions to trauma that warrant understanding and sensitive care).[60] In addition, adults can learn key strategies to manage trauma-related problems in childhood. These include creating environments that feel physically and emotionally safe; teaching children self-regulation, language and communication skills, and how to build healthy relationships; learning each child’s trauma triggers and how both the child and adults can limit, anticipate, and cope with them; and supporting the development of healthy attachments with parents and other caregivers, as well as positive relationships with peers. Evaluations of TIC initiatives also indicate that when parents, service providers, and programs share a common language and view of trauma, they are better able to work together to meet children’s needs.[61]
Training and professional development opportunities are also important for increasing the capacity of adults to attend to other aspects of TIC, including family engagement; practices that are responsive to culture, gender, and sexual orientation; collaboration with community service providers (e.g., mental health providers who can screen for childhood trauma and provide evidence-based treatment); developing and integrating emergency and crisis response protocols; and establishing trauma-informed policies that support positive youth development despite exposure to trauma. Building capacity and maintaining an ongoing commitment to TIC efforts are critical to sustainability.[62], [63] However, although it is a critical component of TIC, training staff and parents on the impact of childhood trauma is not sufficient and does not in and of itself constitute TIC. TIC must also include comprehensive, ongoing professional development and education for parents, families, school staff, out-of-school program staff, and community service providers on jointly addressing childhood trauma.
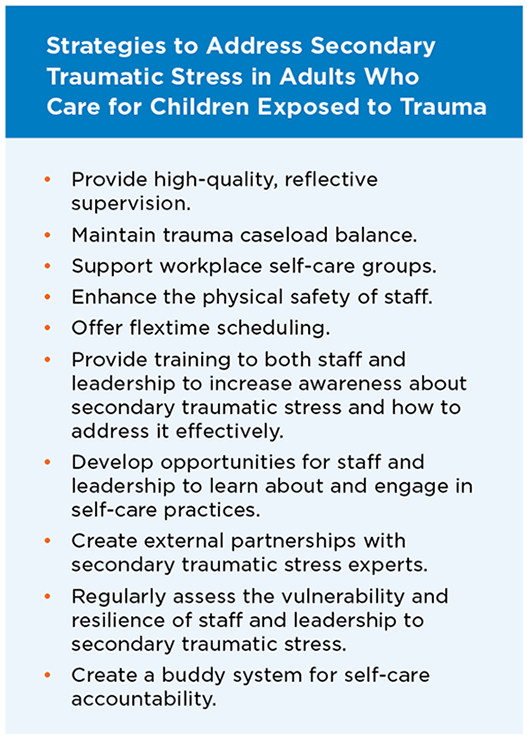
Parents and service providers who work with children who experience trauma require self-care to prevent and mitigate the effects of secondary traumatic stress. TIC also means attending to the psychological and physical safety and well-being of the adults who care for children who have experienced trauma.[64], [65] Professionals, parents, and other caregiving adults may suffer secondary traumatic stress (trauma-related reactions to exposure to another person’s traumatic experience).[66],[67] Psychoeducation (helping others understand the impact of trauma, both on affected individuals and on their service providers, as well as pathways toward recovery),[68] skills training, high-quality supervision, and self-care (e.g., rest, exercise, social support, mindfulness and other stress reduction activities, engaging in pleasurable activities and hobbies, psychotherapy) are critical to ensuring adult well-being and providing sufficient personal resources to work effectively with children who are exposed to trauma. See Figure 4 for specific strategies recommended by the National Child Traumatic Stress Network to combat secondary traumatic stress and reduce related staff burnout and turnover.[69]
Further research is needed on TIC in child-serving programs, institutions, and systems to develop a sufficient evidence base to inform policy and practice. TIC is a relatively new framework for working with individuals who experience trauma, and the evidence base in support of its effectiveness is in the early stages of development. However, a number of promising TIC initiatives in early care and education, schools, child welfare, and behavioral health have demonstrated improvements in trauma-related knowledge and skills among service providers, foster parents, and family members; reductions in children’s posttraumatic stress symptoms and problem behaviors; and increases in children’s strengths and protective factors.[70],[71],[72],[73],[74] In addition, a growing number of clinical treatment models—including Trauma-Focused Cognitive Behavioral Therapy,[75],[76] Child-Parent Psychotherapy,[77],[78] Attachment and Biobehavioral Catch-up,[79],[80] and Parent-Child Interaction Therapy,[81],[82]—have undergone rigorous evaluation and shown positive outcomes for children from infancy to late adolescence. However, TIC is not limited to mental health professionals. Each child-serving program, institution, or service system can play a role in TIC, including referral to clinical treatment and follow-up with families.
Conclusion
Trauma-informed programs, institutions, and service systems are critical to promoting and fostering resilience in all children, and particularly those who have experienced trauma. TIC requires comprehensive, multi-pronged support from adults in all aspects of children’s lives. It includes increasing adults’ knowledge of childhood trauma and helping them recognize the symptoms, as well as giving them the resources to support and refer children who have experienced trauma to appropriate services. Additionally, as programs make their services more trauma-informed, it is important that they promote self-care to prevent or address secondary trauma among adults working with children who have experienced trauma.
Endnotes
[1] De Bellis, M. D. & Zisk, A. (2014). The biological effects of childhood trauma. Child and Adolescent Psychiatric Clinics of North America, 23(2), 185-222.
[2] Enlow, M., Blood, E., & Egeland, B. (2013). Sociodemographic risk, developmental competence, and PTSD symptoms in young children exposed to interpersonal trauma in early life. Journal of Traumatic Stress, 26(6), 686–694.
[3] Lieberman (2004). Traumatic stress and quality of attachment: Reality and internalization in disorders of infant mental health. Infant Mental Health Journal, 25(4), 336–351.
[4] National Child Traumatic Stress Network. (2003). Complex trauma in children and adolescents: White paper from the National Child Traumatic Stress Network Complex Trauma Task Force. Los Angeles, CA and Durham, NC: National Center for Child Traumatic Stress. Retrieved on February 3, 2017 from https://www.nctsn.org/sites/default/files/resources//complex_trauma_in_children_and_adolescents.pdf
[5] Substance Abuse and Mental Health Services Administration. SAMHSA’s concept of trauma and guidance for a trauma-informed approach. HHS publication no. (SMA) 14-4884. Rockville, MD: Substance Abuse and Mental Health Services Administration.
[6] International Society for Traumatic Stress Studies. (n.d.). What is childhood trauma? Retrieved June 8, 2018 from http://www.istss.org/public-resources/remembering-childhood-trauma/what-is-childhood-trauma.aspx
[7] Substance Abuse and Mental Health Services Administration-Health Resources & Services Administration. (n.d.). Adverse childhood experiences (ACES), trauma, & Post Traumatic Stress Disorder (PTSD). Retrieved June 8, 2018 from https://www.integration.samhsa.gov/clinical-practice/trauma#ACE_Trauma_PTSD_Resources
[8] The National Child Traumatic Stress Network. (n.d.). What is child trauma? Retrieved June 8, 2018 from https://www.nctsn.org/what-is-child-trauma
[9] National Child Traumatic Stress Network (n.d.). Trauma types. Retrieved on June 8, 2018 from https://www.nctsn.org/what-is-child-trauma/trauma-types
[10] National Survey of Children’s Health. (2011/12). Data query from the Child and Adolescent Health Measurement Initiative, Data Resource Center for Child and Adolescent Health website. Retrieved June 8, 2018 from www.childhealthdata.org.
[11] U.S Department of Health & Human Services Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2019). Child maltreatment 2017. Washington, DC: Children’s Bureau. Retrieved June 8, 2018 from https://www.acf.hhs.gov/cb/resource/child-maltreatment-2017
[12] McLaughlin, K. A., Koenen, K. C., Hill, E. D., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., & Kessler, R. C. (2013). Trauma exposure and posttraumatic stress disorder in a US national sample of adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 52, 815-830.
[13] U.S. Department of Health & Human Services Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2019).
[14] Grossman, G. (2000). The history of injury control and the epidemiology of child and adolescent injuries. The Future of Children, 10(1), 23-52.
[15] Fantuzzo, J., & Fusco, R. (2007). Children’s direct exposure to types of domestic violence crime: A population-based investigation. Journal of Family Violence, 22(7), 543-552.
[16] Slopen, N., Shonkoff, J. P., Albert, M. A., Yoshikawa, H., Jacobs, A, Stoltz, R., & Williams, D. R. (2016). Racial disparities in child adversity in the U.S.: Interaction with family immigration history and income. American Journal of Preventive Medicine, 50(1), 47-56.
[17] De Bellis, M. D., & Zisk, A. (2014). The biological effects of childhood trauma. Child and Adolescent Psychiatric Clinics, 23(2), 185-222.
[18] Enlow, M. B., Egeland, B., Blood, E. A., Wright, R. O., & Wright, R. J. (2012). Interpersonal trauma exposure and cognitive development in children to age 8 years: a longitudinal study. Journal of Epidemiological Community Health, 66(11), 1005-1010.
[19] Shonkoff, J. P., Boyce, T., & McEwen, B. S. (2009). Neuroscience, molecular biology, and the childhood roots of health disparities: building a new framework for health promotion and disease prevention. JAMA, 301(21), 2252-2259.
[20] Streeck-Fischer, A., & van der Kolk, B. A. (2000). Down will come baby, cradle and all: Diagnostic and therapeutic implications of chronic trauma on child development. Australian and New Zealand Journal of Psychiatry, 34, 903–918.
[21]National Child Traumatic Stress Network. (2003).
[22] U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment. (2014). Trauma-informed care in behavioral health services: Treatment Improvement Protocol (TIP) Series, No. 57. HHS Publication No. (SMA) 14-4816. Rockville, MD: Author.
[23] Child Trends DataBank. (2013). Adverse experiences. Retrieved on June 8, 2018 from: https://www.childtrends.org/indicators/adverse-experiences
[24] American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
[25] American Psychological Association Presidential Task Force on Posttraumatic Stress Disorder and Trauma in Children and Adolescents. (2008). Children and trauma: Update for mental health professionals. Washington, DC: American Psychological Association. Retrieved May 7, 2019 from http://www.apa.org/pi/families/resources/update.pdf
[26] Teicher, M. H., Andersen, S. L., Polcari, A., Anderson, C. M., & Navalta, C. P. (2002). Developmental neurobiology of childhood stress and trauma. Psychiatric Clinics of North America, 25(2), 397–426.
[27] The National Child Traumatic Stress Network. (2010). Age-related reactions to a traumatic event. Los Angeles, CA and Durham, NC: National Center for Child Traumatic Stress. Retrieved March 19, 2019 from https://www.nctsn.org/sites/default/files/resources//age_related_reactions_to_traumatic_events.pdf
[28] Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71(3), 543-562.
[29] Masten, A. S. (1994). Resilience in individual development: Successful adaptation despite risk and adversity. In M. C. Wang & E. W. Gordon (Eds.), Educational resilience in inner-city America: Challenges and prospects (pp. 3-25). Hillsdale, NJ: Lawrence Erlbaum Associates.
[30] Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5(1), 25338.
[31] The National Child Traumatic Stress Network. (n.d.). Core curriculum on childhood trauma. Retrieved on June 8, 2018 from https://www.nctsn.org/treatments-and-practices/core-curriculum-childhood-trauma
[32] World Health Organization. Risk factors. Retrieved on June 8, 2018 from http://www.who.int/topics/risk_factors/en/
[33] Smart, J. (2017). Risk and protective factors for child abuse and neglect. Australia: Australian Institute of Family Studies, Child Family Community Australia. Retrieved March 19, 2019 from
https://aifs.gov.au/cfca/publications/risk-and-protective-factors-child-abuse-and-neglect
[34] Child Welfare Information Gateway. (2004). Risk and protective factors for child abuse and neglect. Washington, DC: Administration for Children and Families, U.S. Department of Health and Human Services. Retrieved March 19, 2019 from https://www.childwelfare.gov/pubPDFs/riskprotectivefactors.pdf
[35] Smart, J. (2017).
[36] McCormick, A., Scheyd, K., & Terrazas, S. (2018). Trauma-informed care and LGBTQ youth: Considerations for advancing practice with youth with trauma experiences. Families in Society, 99(2), 160-169.
[37] Sogomonyan, F. & Cooper, J. L. (2010). Trauma faced by child of military families: What every policymaker should know. New York, NY: National Center for Children in Poverty. Retrieved March 19, 2019 from http://www.nccp.org/publications/pub_938.html
[38] National Center for Mental Health Promotion and Youth Violence Prevention, Safe Schools Healthy Students. (2004). Risk and resilience 101. Washington, DC: Education Development Center. Retrieved March 19, 2019 from http://www.promoteprevent.org/sites/www.promoteprevent.org/files/resources/Risk%20and%20Resilience.pdf
[39] Smart, J. (2017).
[40] National Scientific Council on the Developing Child (2005/2014). Excessive stress disrupts the architecture of the developing Brain: Working paper no. 3. Updated edition. Retrieved March 19, 2019 from www.developingchild.harvard.edu
[41] Bartlett, J. D., Smith, S., & Bringewatt, E. (2017). Helping young children who have experienced trauma: Policies and strategies for early care and education. Bethesda, MD: Child Trends. Retrieved March 19, 2019 from https://cms.childtrends.org/wp-content/uploads/2017/04/2017-19ECETrauma.pdf
[42] Blaustein, M. & Kinniburgh, K. (2010). Treating traumatic stress in children and adolescents: How to
[43] Lieberman, A. (2004).
[44] National Scientific Council on the Developing Child. (2015).
[45] The National Child Traumatic Stress Network. (2016). Resilience and child traumatic stress. Los Angeles, CA and Durham, NC: National Center for Child Traumatic Stress. Retrieved March 19, 2019 from https://www.nctsn.org/sites/default/files/resources//resilience_and_child_traumatic_stress.pdf
[46] Center for the Study of Social Policy. (n.d.). Protective factors framework. Washington, DC: Center for the Study of Social Policy. Retrieved March 19, 2019 from https://cssp.org/our-work/projects/protective-factors-framework/
[47] SAMHSA’s concept of trauma and Guidance for a trauma-informed approach. HHS publication no. (SMA) 14-4884. Rockville, MD: Author.
[48] Bronfenbrenner, U., & Morris, P. A. (2006). The bioecological model of human development. In R. M. Lerner & W. Damon (Eds.), Handbook of child psychology: Theoretical models of human development (pp. 793-828). Hoboken, NJ: John Wiley & Sons.
[49] Substance Abuse and Mental Health Services Administration. (2014).
[50] Elliott, D. E., Bjelajac, P., Fallot, R. D., Markoff, L. S., & Reed, B. G. (2005). Trauma-informed or trauma-denied: Principles and implementation of trauma-informed services for women. Journal of Community Psychology, 33, 461–477 (p. 467).
[51] Substance Abuse and Mental Health Services Administration. (2014).
[52] Substance Abuse and Mental Health Services Administration. (2014).
[53] Baird, K., & Kracen, A. C. (2006). Vicarious traumatization and secondary traumatic stress: A research synthesis. Counselling Psychology Quarterly, 19(2), 181-188.
[54] Substance Abuse and Mental Health Services Administration. (2014).
[55] Substance Abuse and Mental Health Services Administration. (2014).
[56] Substance Abuse and Mental Health Services Administration. (2014)..
[57] Substance Abuse and Mental Health Services Administration. (2014).
[58] Green Cross Academy of Traumatology. (2007). Standards of traumatology practice revised. http://www.greencross.org/index.php?option=com_content&view=article&id=183&Itemid=123
[59] 3. Lang, J., Campbell, K., & Vanderploeg, J. (2015) Advancing trauma-informed systems for children. Farmington, CT: Child Health and Development Institute of Connecticut. Retreived March 30, 2017 from www.chdi.org/files/7514/4405/4524/Trauma_IMPACT_-_FINAL.pdf
[60] Cole, S. F., Eisner, A., Gregory, M. & Ristuccia, J. (2013). Helping traumatized children learn: Creating and advocating for trauma-sensitive schools (Vol. 2). Boston, MA: Massachusetts Advocates for Children. Retrieved March 19, 2019 from from https://traumasensitiveschools.org/wp-content/uploads/2013/11/HTC
L-Vol-2-Creating-and-Advocating-for-TSS.pdf
[61] Bartlett, J. D., & Rushovich, B. (2018). Findings on the implementation of Trauma Systems Therapy Foster Care (TST-FC) in child welfare. Children & Youth Services Review, 91, 30-38.
[62] Substance Abuse and Mental Health Services Administration. (2014).
[63] The National Child Traumatic Stress Network. (n.d.). Essential elements of a trauma-informed school system. Retrieved on June 8, 2018 from https://www.nctsn.org/trauma-informed-care/trauma-informed-systems/schools/essential-elements
[64] Baird, K., & Kracen, A. C. (2006)
[65] The National Child Traumatic Stress Network. (n.d.). Introduction. Retrieved on June 8, 2018 from https://www.nctsn.org/trauma-informed-care/secondary-traumatic-stress/introduction
[66] Substance Abuse and Mental Health Services Administration. (2014).
[67] Baird, K., & Kracen, A. C. (2006)
[68] The role of psychoeducation in trauma and recovery: Recommendations for content and delivery. Journal of Evidence-Informed Social Work, 13(5), 442-451.
[69] The National Child Traumatic Stress Network. (n.d.). Introduction. Retrieved March 30, 2017 from
https://www.nctsn.org/trauma-informed-care/secondary-traumatic-stress/introduction
[70] Bartlett et al. (2017).
[71] Bartlett, J. D., Griffin, J.L., Spinazzola, J., Goldman Fraser, J., Noroña, C.R., Bodian, R., … Barto, B. (2018). The impact of a statewide trauma-informed care initiative in child welfare on the well-being of children and youth. Children & Youth Services Review, 84, 110-117.
[72] Barto, B., Bartlett, J. D., Bodian, R., Noroña, C. R., Spinazzola, J., Griffin, J. L., … Todd, M. (in press). The impact of a statewide trauma-informed child welfare initiative on children’s permanency and maltreatment outcomes. Children & Youth Services Review.
[73] Lang et al. (2015)..
[74] Wright, T. (2014). Too scared to learn: Teaching young children who have experienced trauma: Research in review. Young Children, 69(5), 88–93.
[75] Cohen, J. A., Mannarino, A. P., & Deblinger, E. (2006). Treating trauma and traumatic grief in children and adolescents. New York: Guilford Press.
[76] Cohen, J. A., Mannarino, A. P., & Knudsen K. (2005). Treating sexually abused children: One year follow-up of a randomized controlled trial. Child Abuse & Neglect, 29, 135-146.
[77] Lieberman, A. F., & Van Horn, P. (2004). Don’t hit my mommy: A manual for child parent psychotherapy with young witnesses of family violence. Zero to Three Press: Washington, D.C.
[78] Lieberman, A. F., Ghosh Ippen, C., & Van Horn, P. (2006). Child-Parent Psychotherapy: 6-month follow-up of a randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 45(8), 913-918.
[79] Dozier, M., Lindhiem, O., & Ackerman, J. (2005). Attachment and biobehavioral catch-up. In L. Berlin, Y. Ziv, L. Amaya-Jackson, & M. T. Greenberg (Eds.), Enhancing early attachments (pp. 178-194). New York: Guilford.
[80] Dozier, M., Peloso, E., Lindhiem, O., Gordon, M. K., Manni, M., Sepulveda, S., … & Levine, S. (2006). Developing evidence-based interventions for foster children: An example of a randomized clinical trial with infants and toddlers. Journal of Social Issues, 62(4), 767-785.
[81] Eyberg, S.M., Funderburk, B. W., Hembree-Kigin, T., McNeil, C. B., Querido, J., & Hood, K.K. (2001). Parent-child interaction therapy with behavior problem children: One- and two-year maintenance of treatment effects in the family. Child & Family Behavior Therapy, 23, 1-20.
[82] Chaffin, M., Silovsky, J. F., Funderburk, B., Valle, L. A., Brestan, E. V., Balachova, T., … Bonner, B. (2004). Parent-Child Interaction Therapy with physically abusive parents: Efficacy for reducing further abuse reports. Journal of Consulting and Clinical Psychology, 72(3), 500-510.
© Copyright 2025 ChildTrendsPrivacy Statement
Newsletter SignupLinkedInYouTubeBlueskyInstagram