

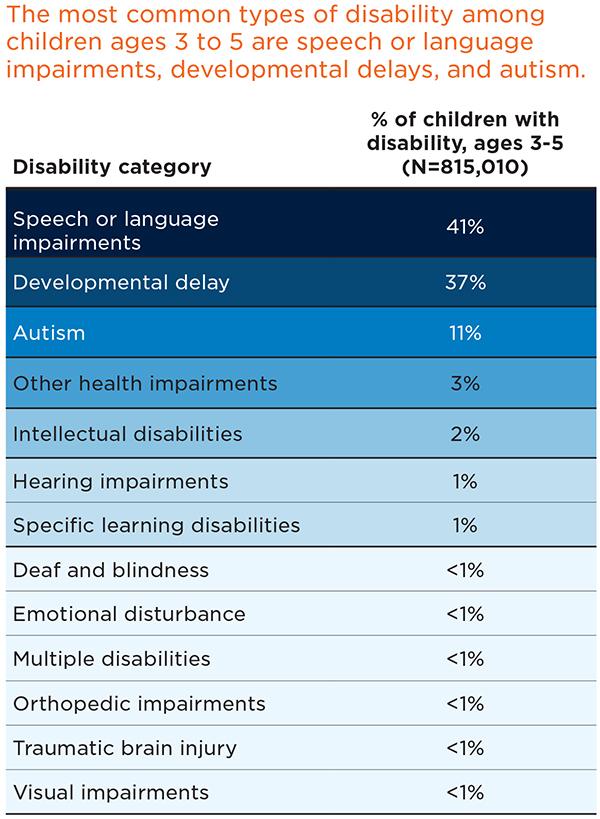
Coping with the COVID-19 pandemic has been challenging for all families, especially those caring for young children with disabilities. Of the 24 million children under age 6 in the United States, about 5 percent (1.2 million) have a diagnosed disability, which qualifies them for early intervention or special education services through the Individuals with Disabilities Education Act (IDEA).1 IDEA categorizes 13 different types of disabilities in children, including conditions such as autism spectrum disorder, speech or language impairment, visual impairment, deafness, intellectual disabilities, and other specific learning disabilities (i.e., dyslexia or auditory processing disorder). As a result of the pandemic, these children and their families may face challenges beyond those faced by other families.
This fact sheet examines the interrelationship between disability, race, and ethnicity, and how this plays out across the country. Next, it discusses specific impacts of the pandemic on families with young children with disabilities, and, finally, the resource offers considerations for states as ECE programs begin to reopen.
Background
Access to early intervention and early childhood special education is critical to child development and learning for children with disabilities. IDEA services are individualized to each child’s needs and goals are set by their family and by practitioners and educators. Children are regularly assessed to gauge their progress toward meeting goals. For infants and toddlers, services are delivered in a “natural environment,” including at home, in an early care and education (ECE) program, or within another setting in the community. Preschool children with disabilities are entitled to a free and appropriate education (sometimes referred to as FAPE) in a “least restrictive environment.” In other words, children with disabilities receive services in many of the same settings as typically developing children their age. They rely on child care programs, Head Start, and schools to be open and accessible to receive services that support their development and learning. When COVID-19 forced many of these ECE programs to close, access to many of these services was cut off.
Not only do ECE programs frequently support young children with disabilities via early intervention and special education services, they also play an important role in early identification of developmental delays for children without official diagnoses. ECE programs may provide or refer families to developmental screening, and they help plan for ways to enhance that child’s development and for their full inclusion in the program. When ECE programs close, children with disabilities, or those who are at risk for developmental delays, are left without a resource that is critical to their daily life and long-term development and well-being.
Disability’s intersection with race and ethnicity
Across states, the proportion of children participating in early intervention and early childhood special education varies (download appendix table), with children in certain racial and ethnic groups having differential access to IDEA services.
Receipt and denial of early intervention and early childhood special education is not a straightforward issue. A substantial body of evidence documents the relationship between race, ethnicity, and disability status, noting that children of color have simultaneously been under- and overrepresented in terms of disability identification.2 These inequities are based on many factors, including programmatic issues such as prejudice and biases among service providers,3 a lack of culturally sensitive approaches, and language barriers.4,5,6,7 Structural issues—such as less access to health care and insurance,8 and education settings that are segregated by geography and/or disability status9—also come into play and most often have negative implications for communities of color.
The complex interplay of these factors makes it challenging to evaluate whether the under- or overrepresentation of children of color is accurate or appropriate. All of this becomes even more problematic when coupled with the challenges that the COVID-19 pandemic has brought to the fore.
Download
Source: https://www2.ed.gov/programs/osepidea/618-data/static-tables/index.html#partb-cc (Static Tables, Child Count, Part B, Table 2)
Impact of COVID-19
As states respond to the needs of young children with disabilities during the pandemic, it is important to understand that the ECE system in the United States is quite fragmented, essentially rendering it a “non-system.”10 Multiple agencies regulate and fund ECE programs, leading to different guidance being given and enacted across states in ECE programs. School districts, referred to as local education agencies (LEAs), are part of the ECE network and frequently serve young children with disabilities. Much of the COVID-19 response guidance followed by LEAs comes from federal and state agencies,11,12,13 but confusion still exists. For example, there have been recent reports of LEAs inappropriately asking families to waive their rights to services,14 and about 40 percent of families with a child receiving special education report they are not receiving the services designated in their child’s individualized education plan (IEP).15 In addition, because of the multiple levels of ECE management, it is challenging for states and programs to monitor and respond in a unified way to potential disparities related to race, ethnicity, and/or disability status. The confluence of a fragmented ECE system (undergirded by racial and ethnic disparities), and the COVID-19 pandemic, impact children and families in a number of ways.
Loss of in-person therapy services. One of the more immediate changes for a young child with a disability is the sudden loss of in-person therapy services. Due to social distancing guidelines, some of these services have shifted to telehealth formats,16 but other services simply are not possible in a virtual format. For example, physical and occupational therapy rely on specialized equipment that may not be readily available in a family’s home. Even when families have access to this equipment, they may not have the ability to use it.
Limited access to special education accommodations and adapted materials. Similarly, young children enrolled in ECE programs have lost in-person special education accommodations. One important role of early interventionists and early childhood special educators is the development and adaptation of play-based and educational activities to accommodate the specific needs of a young child with a disability. In a distance learning environment or a remote early intervention session, certain adaptations may be difficult or impossible to make. For example, children in social skills groups may no longer be able to engage in therapeutic play with their peers. With the loss of access to in-person ECE professionals and adaptive technologies in ECE programs, young children with disabilities and their families struggle to keep up routines.
Difficulty of taking on new roles for therapy and learning within families. A further challenge for remote services and distance learning is that families are now tasked with supporting children’s learning, but typically lack expertise in special education, an in-depth understanding of how to adapt activities, or the ability to navigate technology to meet their child’s needs. For instance, children previously supported by one-to-one special education paraprofessionals (special education paraprofessionals’ average caseloads range from 15 to 23 students)17 now rely on parents or other adult caregivers in their homes. Further, many parents must now take on new roles in educating and supporting their child while simultaneously working.
Compounded social isolation for families of young children with disabilities. Prior to COVID-19, families of young children with disabilities already experienced more social isolation than other families (e.g., lack of travel opportunities, long bouts of hospitalization, lack of time and energy due to caregiving responsibilities).18 During the COVID-19 pandemic, the risk of isolation has been compounded by social distancing mandates. Families who previously tapped into extended family member networks, or who paid caregivers and programs to provide social supports and/or respite care, may now be isolated. Further, families who have young children with medical issues that compromise their immune systems face daunting decisions about who can come into or leave the home, and how to mitigate the risks of catching the virus in the community.
Gaps in health insurance coverage for children with unemployed parents. One in six American workers (about 30 million) have filed unemployment claims since the pandemic began.19 Young children with disabilities who have health insurance coverage through their parent’s employer may face a loss of coverage for therapy services and supports. This is particularly challenging for young children with disabilities who receive frequent therapy services or who require regular medical appointments to treat complex medical conditions.
Action steps for state policymakers
As states plan the reopening of ECE settings, they must also plan to equitably include young children with disabilities. We offer the following examples of action steps that can support a strong return to services and ensure that young children with disabilities receive support for their development and learning.
Partner with experts. Include the voices of families, providers, therapists, and child development scientists when making plans for a reopening that meets the needs of young children with disabilities. Each stakeholder group brings perspectives that can ground plans in the needs of children with disabilities and their families and help young children connect and/or reconnect with services that support their growth and development.
Partner across state agencies. Prioritize information sharing and partnerships across state agencies that set guidelines for programs that support young children with disabilities. For example, state agencies can ensure consistency in any waivers for families or programs, set consistent re-entry guidelines across settings, and establish public health communication strategies that include reminders about young children with disabilities, their needs, and their rights to be included.
Provide guidance for ECE programs. When developing guidelines for reopening, include considerations for ECE programs that care for young children with disabilities. For example, these programs may need additional guidance on preventing transmission of COVID-19 in ways that do not isolate children with disabilities from their peers, therapists, and support personnel.
Consider in-home services. Parents may need or want to keep their young children at home, rather than return them to a formal child care setting, to reduce the risk of transmission. Include strategies for ensuring service delivery to these families.
Include time to reestablish goals and conduct assessments. As young children with disabilities transition back into services and care, make sure that all staff involved with the family—therapists, teachers, paraprofessionals, and administrators—discuss what supports the child may have received while away from care. Staff should make plans for moving forward that account for the ongoing needs of the child and for available services.
Increase mental health supports. During and after the pandemic, families and children may face a myriad of stressors, such as the loss of a family member or friend due to the illness, their fear of infection, loss of income, and the need to juggle conflicting work and caregiving responsibilities. Programs may require that internal staff or staff from community partner organizations support young children with disabilities who are dealing with increased anxiety and social acclimation challenges, in addition to their underlying disability.
Plan for additional closures and disruption of services. Although states are moving ahead with phased reopenings, there is a chance that states, communities, or individual providers will need to reclose or limit in-person services again if infections spike. Include young children with disabilities in those plans, and account for their unique needs, to ensure the most continuous service delivery possible.
Child Trends Resources
- COVID-19’s forgotten children
- Children with special health care needs face challenges accessing information, support, and services
- Children with special health care needs are more likely to have adverse childhood experiences
- A state multi-sector framework for supporting children and youth with special health care needs
- 5 things to know about racial and ethnic disparities in special education
Policy Guidance Resources
- Office of Special Education Programs (OSEP) COVID-19 Guidance Q&A
- Office of Head Start COVID-19 Guidance
Other Resources
References
Download
© Copyright 2025 ChildTrendsPrivacy Statement
Newsletter SignupLinkedInYouTubeBlueskyInstagram